I got a link to the new American Psychiatric Association (APA) Practice guideline today in my Facebook feed. It was entitled Practice Guidelines for the Psychiatric Evaluation of Adults. It is an updated version of a previous guideline by the same name. I have pointed out on this blog that the APA seems to have all but abandoned the production of these guidelines with the exception of some extensive work for CMS to determine whether or not administrative guidelines about billing and coding were adequate. When I complained to APA officials about the fact that they were not producing any new or updated guidelines I was told two things. The first was to wait for this current guideline. The second was that guideline production and updating did not seem to be a wise use of limited resources. My interpretation of that remark was that it was defeatist and probably related to the fact that everyone is currently producing guidelines. I guess that nobody at the APA recognizes the need to set limits on pro-business and pro-government guidelines that actively discriminate against psychiatrists and their patients. Apart from a single APA President, that seems to have been the conventional wisdom that they have been using for the past 30 years.
I read the entire relevant section of the Guideline and that involves the first 52 of 170 pages. The last section includes references, abstracts and methodology like bar graphs showing how many experts agreed that a certain type of assessment needed to be done in an initial assessment. The introductory release explained that the guideline was based on an Institute of Medicine (IOM) publication entitled Clinical Practice Guidelines We Can Trust. I have not been impressed with some of the work done by the IOM in the past and after reading three of their previous books wonder if it makes sense to read a fourth. There are additional references on the methodology in the introductory sections of the document. The release describes the guideline as modular so that each of the nine different modules can be updated regularly and separately. That is a good idea that will hopefully add timeliness to the process. One of the goals is to have the guideline widely disseminated. Apparently anyone can download the document and read it. There are the usual legal qualifiers pointing out the limitations of a broad document like this one and why it cannot be considered a standard of care. I did not see the most obvious reason mentioned and that is that this concept is a legal one used for the determination of medical malpractice and that it really has no application in medicine. Guidelines are referenced in Gutheil and Appelbaum's text: "Third, another source of information about standards of care is the growing number of practice guidelines......... It must be remembered, however, that even well-designed guidelines do not necessarily address all possible approaches to a clinical issue." (1). So the guideline disclaimer is clearly debatable in court.
As I read through the guidelines several things jumped out at me.
1. It was not clear that this guideline was written for psychiatrists - Some may say that this is implicit, but I am bothered by the fact that in the first 52 pages the word "clinician" pops up 34 times and the word "psychiatrist" pops up 17 times. What would prevent any clinician from claiming that they have done everything listed in this document and therefore their evaluation is the equivalent of a psychiatrist's evaluation. This is more than a guild or political issue as I will elaborate below.
2. It was not clear what type of expertise was necessary to use the guideline - I suppose this is a minor variation of the first point, but technical expertise to me has always been a critical issue. The guideline gets around this by saying it is not a "comprehensive" document. I would not consider the recognition of acute medical and neurological problems or even chronic ones to be beyond the scope of a psychiatric evaluation. I would not consider an abbreviated list of these conditions to necessarily render this a comprehensive document and it would certainly have more clinical value than a tedious list of all of the survey results. The document also discusses tests in terms of the optimal ordering of tests and also specific kinds of tests. What about who interprets those tests? As a very basic example, I would go back to the days of the oral board exam in psychiatry and frequent questions about the use of lithium. Board examiners were interested in what tests needed to be ordered to initiate and follow lithium maintenance therapy. The goal of that exercise was to certify a safe practitioner of psychiatry. In today's world, there is a much larger number of tests, interpretations and plans based on those tests. This is a critical line of demarcation in some practice settings that seek to limit the medical role of psychiatrists.
It is apparent that the APA wants this guideline to be widely disseminated. A related concern is that they may have not learned much from the wide dissemination of the DSMs over the years. Although there is a partial financial incentive with DSM releases, the APA may be oblivious to the downside of everyone having a copy of this manual. The pre-DSM-5 release rhetoric illustrates that a lot of critics had a very poor understanding of what the DSM-5 was and how it would be used. Wide dissemination of a vaguely written practice guideline may have the same effect. There is a common bias than anyone with a social brain who can speculate about the motivations and goals of others can do what psychiatrists do. There are endless examples of various writers speculating about which public figure may have Asperger's or narcissistic personality disorder. The sentiment in some circles seems to be: "If I have a copy of the DSM - I can diagnose people." What is to prevent a similar co-opting of the Practice Guideline?
3. There is nothing really surprising in the document - The assessment techniques are either obvious things that psychiatrists and psychiatric trainees do on a regular basis. There are so many qualifiers that many approaches can be taken. For example, the issue of coming back to an initial point to clarify the diagnosis if it could not be appropriately done in the initial interview was mentioned several times. That is useful in cases when a patient is embarrassed or defensive about a particular aspect of their history. In this regard, the document represents both content and process variables of the interview.
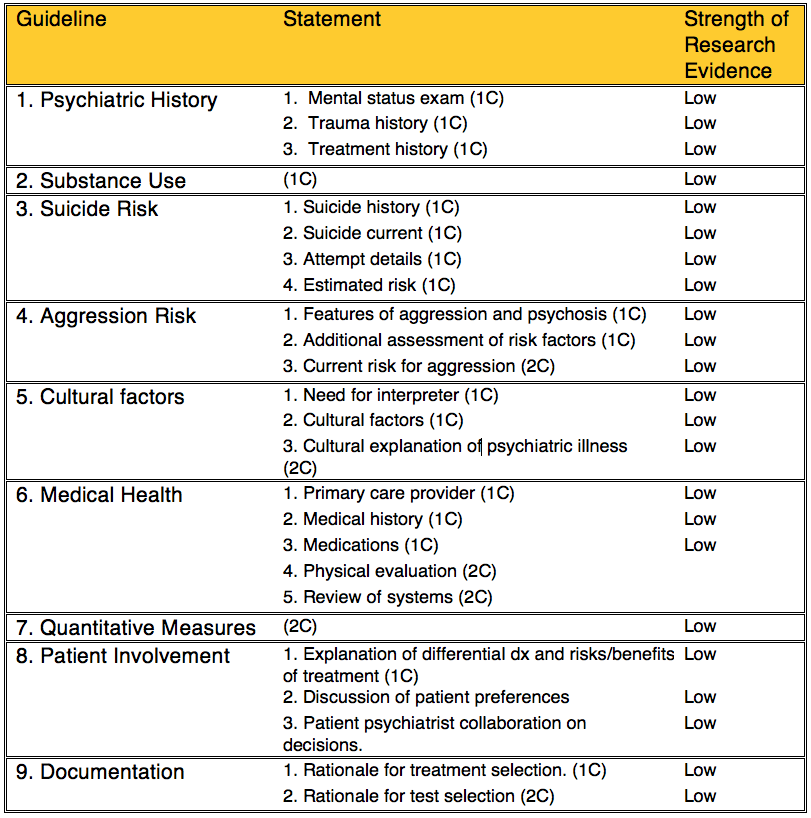
4. Tip of the cap to evidence based medicine - even when it is not needed - A common refrain throughout the guideline was: The strength of research evidence supporting X is low, where X is the guideline of interest. I summarized the guidelines and statements in the table below. The numerical and letter designations can be translated as follows. The numeral 1 is a recommendation. The numeral 2 is a suggestion. The letters A, B, and C are degrees of evidence reflecting high moderate or low degrees of evidence respectively. The table basically reads as a recommendation or a suggestion backed by low degrees of evidence.
Using research evidence as a criteria for standard clinical methods is taking evidence based medicine to its absurd conclusion. I am not talking about refinements in the way the history and physical has been done over the years, but the basic idea that a physician has to make a diagnosis and come up with a treatment plan. Is there really any question that there are currently thousands of clinical trials that document positive treatment effects based on inclusion criteria that include a standard evaluation of the patient and the recognition of certain medical exclusion criteria? The Guideline includes an explanation about why it is unethical to do certain double blind placebo controlled trials such as the study of suicide and aggression. It does not comment on the important clinical question: "When does the anecdotal become statistical?" To illustrate, if I am currently an inpatient psychiatrist and 100% of the patients I see are admitted for suicidal/aggressive ideation/behavior and my post discharge complication rate is very low (1 incident of suicidal or aggressive behavior every 500 discharges) - what is the likelihood that I am no more effective than placebo? Do I really need a clinical trial to prove that I am doing something? Are there any statisticians out there willing to speculate on that problem?
6. A well deserved shot at the electronic health record - After about two decades of hearing nothing but praise for the EHR and how it will revolutionize the practice of medicine and "save" us all hundreds of billions of dollars, its shortcomings are so obvious and so severe that even the APA gets it. From page 44 of the Guideline:
"With the increasing use of electronic record systems, the structured but fragmented information that is common in electronic record notes can increase cognitive workload and reduce the quality of communication among those caring for the patient..."
That is a diplomatic way of saying that if you follow the suggestions for collateral information in the Guideline and are unfortunate enough to get either a printout or have direct access to an EHR, you might spend hours reading through hundreds of pages only to discover that the document has no discharge date, that it contains minimal information or that (in the case of lab testing) you can't determine the dates that any of the testing was done. You will probably also encounter an EHR template approach to documentation that provides a series of "yes-no" responses where real information is traditionally used. The current EHR is a plague on those specialists who require high quality information and plenty of it. It should be apparent from the general requirements of this guideline that psychiatry is at the top of the list.
7. Inconsistencies are present in many places - One of the better examples is several qualifier paragraphs that point out how descriptions may be necessarily vague and how to negotiate that in the assessment itself. There are terms having to do with time as well as clinical descriptions. The guideline says that it does not encourage stereotypical questions to complete the assessment, but at the same time suggests "quantitative measures" like standard checklists. I cringe when I see that term because it was a term that was included in the Joint Commissions 2000 statement on pain assessment and treatment and we all know how that turned out. To an old chemist, asking a person where they are on a ten point scale that rates pain or depression or anxiety is far from a quantitative measurement. At some point, psychiatrists and physicians lost sight of the fact that certain organ systems (the brain in particular) by its very structure, precludes quantitative analysis - and that is a good thing. The authors of this guideline should at least attempt to explain how an obviously subjective and flexible evaluation can eventually lead to rigid "quality" measures that are also being used as if they are quantitative. At some point, some professional organization needs to point out that most if not all of these measures are fabrications of the business community and government and they have little to do with medicine or science. If the APA can say that about all of the points in their guideline, why can't they point out that the same "quantitative measures" are used in collaborative care and they mean the same thing.
8. The serious dimension of the diagnosis - There are a lot of reasons why patients and families tend not to take a psychiatric diagnosis as serious as they should. It took me a number of years in clinical practice before I realized that any informed consent discussion I have with a person should include whether or not that diagnosis is life threatening to them. In some cases like talking with a survivor of a near lethal suicide attempt it is obvious. In other cases like a major psychiatric disorder and a number of close calls due to a substance use disorder, it is less obvious. I will tell a person that the condition they have is life-threatening and the treatment plan and their part in the overall treatment needs to take that into account. There may be an associated discussion of voluntary and involuntary treatment as well as a clarification of my position in the patient's treatment and the associated rationale. I think it is critical that this assessment is made and carefully documented for continuity of care purposes.
These are a few of my initial comments. The new treatment guidelines is far from perfect but it is a start to get the APA back on track again to establish reasonable guidelines written by psychiatrists about the practice of psychiatry. The introductory material suggests that the method will be to modify the various sections, but what is needed is another section or probably a new guideline on treatment planning and how that interfaces with the Evaluation Guideline.
George Dawson, MD, DFAPA
1: APA Work Group on Psychiatric Evaluation. The American Psychiatric Association practice guidelines for the psychiatric evaluation of adults — Third edition. American Psychiatric Association, 2015.
Interesting factoid: A significant p value does not specify the probability that the same result can be reproduced
ReplyDeletein another study.