Showing posts with label CDC. Show all posts
Showing posts with label CDC. Show all posts
Monday, January 15, 2018
A Short (11 minute) Film About Alcoholism - Breakfast Wine
"In Ireland, they say it takes just 3 alcoholics to keep a small bar running in a country town....."
I ran into this film last week and was impressed enough to write this post about it. It is an award winning short film about four people in a pub in rural Ireland and events that transpired on a certain day. Given the availability and brevity of the film, I encourage anyone interested to view the video before reading this post.
You can go to any number of Saturday Night Live skits and see alcoholics ridiculed. This film takes the problem more seriously. What you see will depend on your experience observing and interacting with people who have an alcohol problem.
To set the scene, the film begins with the quote posted at the top of this page. We see two middle-aged men standing outside a pub waiting for it to open. The owner shows up. They all enter and the two men who were waiting commence drinking pints of Guinness. Over the duration of the time lapse in the film they each drink 6 pints of Guinness - the first two in what seems fairly rapid succession.
After they put down about two pints a young woman enters, asks them about the availability of wine. After getting their recommendations she proceeds to drink the first glass rapidly. Over the time lapsed in the film she drinks a total of 4-187.5 ml bottles. The pub owner and the two men in the bar seem impressed with her ability to drink, but they are also impressed with her ability as a ranconteur. She tells a fable about getting rid of all motor transport and lining people up against the wall and shooting them. She moves on to describe severe physical abuse by her husband and shows lacerations on her wrists where she was tied up on the garage floor. She tells them what her husband was saying to her when he became abusive and does not miss a beat. She sarcastically dismisses her rant by saying "I should have seen it coming." At that point she says good bye and the pub owner tells her what the opening time for the pub is every day. She thanks him for the information and walks out. The men are clearly impressed with her and one of them longingly touches the stool where she was sitting.
At the level of entertainment, I can see why this is an award winning short. The writing and acting are good. The woman in the scene, actress Ruth Bradley is a compelling screen presence. She plays this role perfectly. It is a plausible scene from any bar - Irish or American. From the standpoint of an addiction psychiatrist - what is wrong with this picture?
The alcohol consumed per unit time is a red flag. The CDC defines binge drinking as probably occurring if a woman consumes 4 or more drinks or a man consumes 5 or more in 2 hours. The time span of this film may be subject to debate but I counted 6 pints of Guinness per man or 9.6 standard drinks and 750 ml wine (4 - 187.5 ml bottles) or 5 standard drinks for the woman. It is clear from the depiction by the actors that they are drinking these beverages at times like water. In bars or pubs bad things tend to happen when the patrons are binge drinking. Binge drinking alone whether it is associated with a diagnosis of alcohol use problems has associated mortality and morbidity per the CDC site.
There is a high tolerance for unusual behavior in the pub. One of the men leaves and his behavior is discussed among the remaining people. In another scene marking the sixth pint he becomes irate with his associate and that behavior is translated as an acknowledgement that he does want another pint. The woman had two discrete rants about motor vehicles and the violence she has sustained by her husband and immediately resumes a normal even joking manner. The men are intensely interested in this woman, she breaks up their routine, is attractive to them and is charismatic. Their response to her description of the violence she has sustained and even the presentation of her wrist lacerations is definitely muted. No one is interested in the violence or her newly acquired wounds, everyone is interested in moving on as soon as possible.
The dynamic that jumps out at me whether I am listening to heavy drinkers talk about relationships or observing them first hand in bars is grandiosity. Grandiosity can be a feature of mood disorders or narcissism. One theory of grandiosity in narcissism is that there is an inadequate mental representation of affirming objects representing attributes or real relationships in the environment. If people with those attributes are absent or the people present have an inadequate positive affiliation with the person in question they can form their own representations. That leads to grandiosity and narcissism as an amplification of a deficient process with more realistic balances. In alcoholism this can occur as a reaction to the hopelessness of the addiction and its sequelae. As an example, a bar full of middle-aged men with alcoholic liver disease betting on who is going to die first. Sometimes it occurs on a larger scale - the family that supports their father's grandiose statements about drinking himself to death during a hospitalization for recurrent hepatic encephalopathy from alcoholic cirrhosis. The person involved comes across as though they are indestructible - but at a deeper level they cannot reconcile the severity of their illness and their inability to stop drinking.
That is what I think the female character brings to this scene. She is clearly in an abusive marriage that she fled earlier the same day that she comes into the pub. She does not appear to be traumatized at all until she demonstrates the injuries and even then she is loudly mocking her husband and eventually herself: "I should have seen it coming!" The men seem transfixed on this story - unable to challenge it or accept the reality of her status as an abused wife.
I saw one comment posted on the YouTube site from a person who watched this film on an airline flight. He was left thinking about the lives of the people in the film and what happened to them. That is natural enough and something I wondered when I encountered a heavily intoxicated young woman in Boston and tried to help her. To me it is always a lesson in the dynamics of heavy alcohol use. There is an element of intoxication involved, but there is more than that driving a lot of the interpersonal behaviors and what you see happening in a pub or bar.
Defensive behavior about the inability to stop can be part of that.
George Dawson, MD, DFAPA
Sunday, July 16, 2017
OIG Approach To Medicare Part D Opioid Prescribing

The pharmacoepidemiology of opioids in the United States depends on a fragmented approach. I recently posted a CDC study that used a commercial pharmacy database to look at the characteristics of opioid prescribing across individual counties in the United States. In the past week I came across this data brief from the Office of Inspector General (OIG) of the US Department of Health & Human Services. Their database is the 43.6 million beneficiaries of Medicare Part D. Their stated goals are to protect beneficiaries and the community from prescription drug abuse, to prevent diversion and illegal sales, and to protect the program from fraud and unnecessary expense.
Their methodology is unique. They look at prescription drug events (PDE) for all opioids prescribed in 2016 that are paid for by Medicare Part D. Any prescription paid by cash or by another insurer is not counted. Every time a prescription is dispensed and covered by the program a PDE record is sent to CMS (Centers for Medicare and Medicaid Services). In this case they calculated total spending on opioids, total Schedule II and III opioid prescriptions, and a number of parameters that look at total cost. They also determined the the prescriptions per beneficiary, and the average daily morphine equivalent dose (MED). In most of the literature on opioid dosing the milligram morphine equivalents (MME) is a common measure. MME is just the total mg of opioid multiplied by a conversion factor. The MED is basically the same measure but it factors in the total duration of the prescription. As an example for a one day supply of either Vicodin (hydrocodone) 10 mg tabs or Percocet (oxycodone) 5 mg tabs:
hydrocodone: 12 tabs x 10 mg = 120 mg x 1 (conversion factor) = 120 MME or MED
oxycodone: 16 tabs x 5 mg = 80 mg x 1.5 (conversion factor) = 120 MME or MED
In addiction practice these are common doses encountered in the low range of prescription opioid use disorders. I used the brand names for hydrocodone and oxycodone preparations here because that is what people commonly report to me and it typically requires more investigation. For example "Percocet" or "Perc30s" commonly refers to higher dose oxycodone without acetaminophen - a single 30 mg tablet of oxycodone or 45 MME. The authors of this brief do not need to be concerned about those data discrepancies because they are able to get specific claims data.
In terms of outcome data, they looked at all of the prescriptions and cost variables as well. They looked at total exposure. One in three Medicare Part D beneficiaries received at least one opioid prescription. That amounts to 14.4 million people out of a 2016 beneficiary base of 43.6 million people. There were a total of 28.2 million hydrocodone-acetaminophen prescriptions, 5 million oxycodone-acetaminophen prescriptions and 14.8 million tramadol prescriptions. Tramadol is not typically included in opioid studies even though the M1 metabolite is a mu receptor agonist. Tramadol is a prodrug metabolized by CYP2D6, metbolism is necessary to to create M1 and slow metabolizer are less likely to experience the analgesic effect and addiction risk.
Of these beneficiaries 501,008 received high dose opioids (MED > 120 mg/day). The indication here was for noncancer or chronic noncancer pain. Hospice patients and cancer patients were excluded. The most common opioid prescribed in this high dose group was oxycodone 30 mg. The study also defined extreme amounts of opioids as an MED of 240 mg and 69,563 patients received that amount. There were 678 patients receiving high extreme amounts a MED of 1,000 mg for an entire year. The concern with very high levels is whether the prescriptions are indicated and whether they might be diverted. The authors also suggested that fraud could be an issue due to stolen Medicare identification number. They did give an example of a patient who got 62 opioid prescriptions on one year (61 from the same family physician) with an average daily MED of 3,130 mg.
The brief also estimates the degree of doctor shopping or seeking prescriptions from more than one physician and pharmacy. The criteria used for this report was 4 prescribers and 4 pharmacies. A total of 22,308 beneficiaries met that criteria and they also had an average daily MED > 120 mg for a period of three months. They also identified 162 beneficiaries who got opioid prescriptions from 10 different prescribers and 10 different prescribers in the same time period. Even larger number of prescribers and pharmacies were noted in the most extreme cases. That number represents about 0.02% of the total number of beneficiaries using opioids and that is the same order of magnitude of a previous estimate from a large commercial prescription database (4).
Using the estimates of high dose opioids and degree of doctor shopping allowed for an estimate of serious risk of opioid overuse or overdose. The number estimate in that category was 89,843 or about 0.6% of the entire group taking opioids.
The brief also looks at the issue of who is prescribing the opioids. For the 89,843 there were an estimated 115,851 prescribers who wrote at least one of those prescriptions. A total of 401 prescribers were determined to be "far outside the norm". One hundred and ninety eight ordered opioids for patients getting extreme amounts of opioids (MED of 240 mg), 264 ordered opioids for patients who appeared to be doctor shopping, and 61 ordered opioids for patients who were members of both groups. The total number of prescriptions written by prescribers in this group was 256,260 opioid prescriptions. There were 15 prescribers who ordered opioids for > 98 beneficiaries receiving extreme amounts (MED of 240 mg). Of the 401 prescribers with questionable prescribing 1/3 or 133 were nurse practitioners (N=81) or physicians assistants (N=52).
Are there any conclusions possible from this administrative look at opioid prescribing in a subset of Medicare patients? I think that there are a few. My conclusions assume that generalizations from this data are possible:
1. Opioids are commonly prescribed to Medicare recipients - and the vast number of these prescriptions appear to be appropriately managed.
2. A small number of prescribers appear to be responsible for most of the inappropriate prescriptions - and there are some outliers practicing at the extremes in terms of prescribing patterns. Very extreme prescribing described in a few cases would appear to be a function of unnecessary use rather than patients with special needs who require extremely high doses of opioids (MED > 375 mg). That is an important point because concentrations of high dose opioid prescribing is often attributed to the special needs of patients or referral patterns resulting in concentrations of these patients and the need for the prescriber to write prescriptions for these amounts. If this was a case of biological variability - a much larger fraction of the patients who require extreme amounts of opioids.
3. The problem of inappropriate prescriber appears to be easy to follow on the CMS data base - the standard political approach to the opioid epidemic is to blame all doctors and mandate various education programs about opioid prescribing. It should be clear that a minority of physicians or in this case prescribers are problem and there should be a targeted approach. At the very minimum the prescribers in the top 1% of all prescribers or the group who is prescribing extreme amounts of opioids, to people who are probably doctor shopping, or both should be receiving active feedback from CMS.
4. Not counting opioids prescribed for cancer or hospice care is an important omission - This is a problem with very little research or policy making. Patients undergoing end-of-life care are prescribed liberal amounts of opioids for pain relief. There is no question that these patients should have adequate pain relief by whatever medication is necessary. The question is what happens when there are opioids from these prescriptions that the patient never uses? One palliative care study (3) noted that of the hospice care agencies responding to their poll, over a third noted that substance use and diversion were a problem for their agency. Diversion of drugs is known to occur in health care systems where there is monitoring and checks and balances. There are large amounts of opioids out in in-home hospice care settings with much less accountability. A similar study looking at the amounts of opioids prescribed in these settings and what happens to that medication is needed.
5. Opioids are not prescribed in isolation - CMS and the OIG are not medical research organizations. A more comprehensive approach to the problem would look at all of the medications that these patients are receiving and not opioids in isolation. Benzodiazepines frequently accompany opioid prescriptions and in some cases with sedative hypnotics for sleep. Prescribing both compounds can lead to serious and in some cases fatal drug interactions. That would result in an additional category of inappropriate prescribing of opioids.
Although this is an administrative database, it does illustrate how this data can be used for pharmacosurveillance purposes. There was emphasis about the cost of opioid prescribing and the need to prevent fraud from a CMS perspective. The data could also be used to provide valuable feedback to physicians and other prescribers as well as politicians and regulators.
It can be used to counter some myths that seem to exist on both sides.
George Dawson, MD, DFAPA
References:
1: US Department of Health and Human Services: Office of the Inspector General. Opioids in Medicare Part D: Concerns about Extreme Use and Questionable Prescribing. HHS OIG Data Brief OEI-02-17-00250.
2: CDC, “Increases in Drug and Opioid-Involved Overdose Deaths: United States, 2010–2015.” MMWR Morb Mortal Wkly Rep, December 30, 2016, pp. 1445–52. Accessed at https://www.cdc.gov/mmwr/volumes/65/wr/mm655051e1.htm on July 16, 2017
3: Blackhall LJ, Alfson ED, Barclay JS. Screening for substance abuse and diversion in Virginia hospices. J Palliat Med. 2013 Mar;16(3):237-42. doi: 10.1089/jpm.2012.0263. Epub 2013 Jan 5. PubMed PMID: 23289944
Saturday, July 8, 2017
Latest From MMWR On Opioid Prescribing In the USA
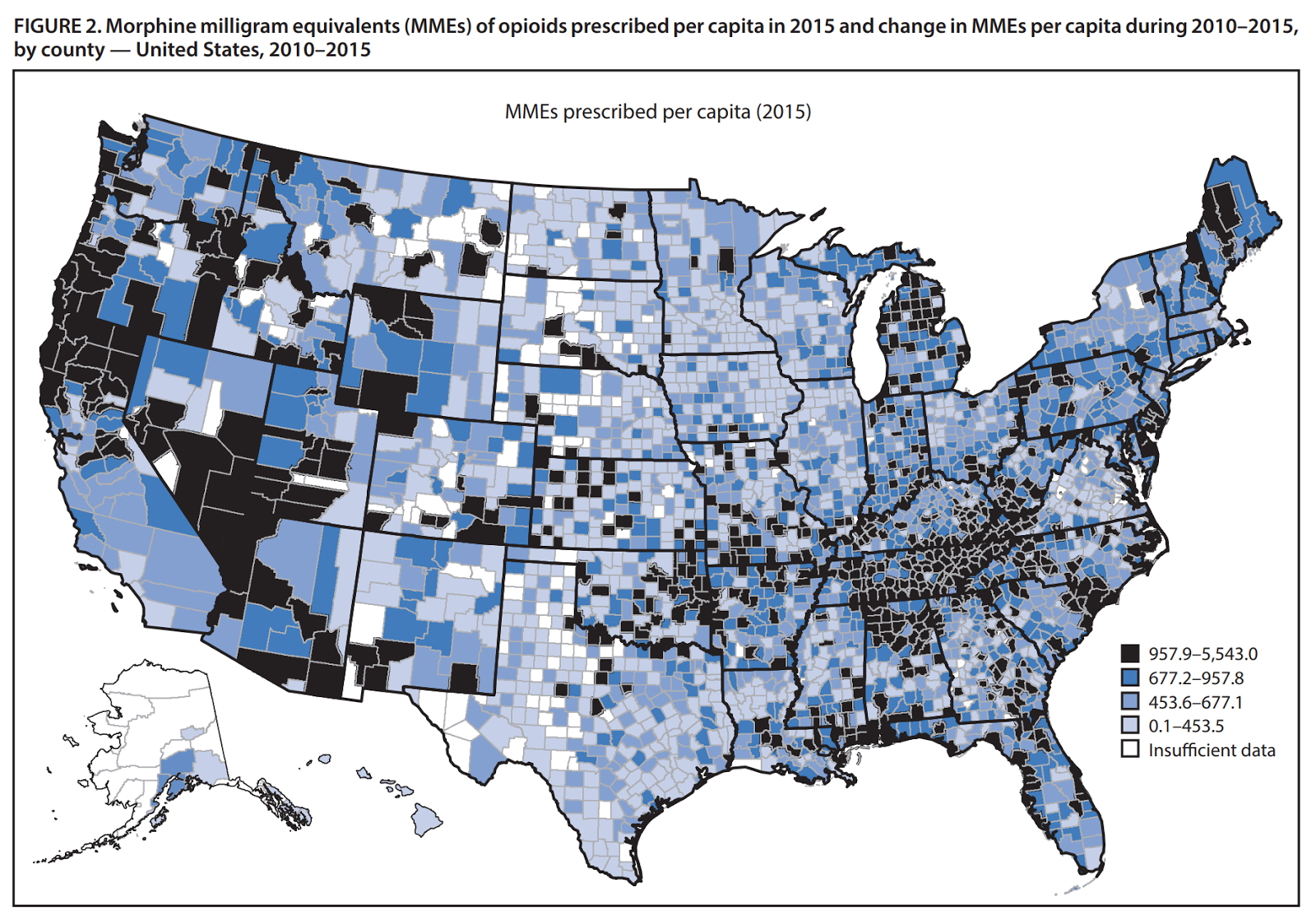
The CDC continues to do outstanding work in providing useful metrics for monitoring the current opioid epidemic. The latest edition of the Morbidity and Mortality Weekly Report is no exception. In this analysis the authors look at a database representing 88% of the opioid prescriptions through retail pharmacies in the USA over the period 2006 to 2015. Buprenorphine products used for medication assisted treatment of opioid use disorder and other preparations containing opioids for non- pain treatment like cough syrups were not included in the total amounts.
They calculated various metrics of interest from the data including the milligram morphine equivalent (MME) per capita and prescribing rates (per 100 persons) for overall rates, high dose rates, and prescribing rates by days of supply given (<30 days or ≥ 30 days). They also looked at county by county rates over the time period studied.
Before I look at the result, I will digress a bit on the MME measure. There are standard conversion charts like this one used by the CDC that allows for conversion of a standard dose of an opioid into a MME. A few examples will illustrate the utility of this conversion. Suppose a person is prescribed oxycodone and acetaminophen tablets. Most of them contain 5 mg oxycodone + 300 mg acetaminophen. If the prescription says to take one tablet 4 times a day of needed for pain that is 20 mg oxycodone total or 20 mg x 1.5 (conversion factor) = 35 MME. Using the same example for hydrocodone (5 mg hydrocodone + 300 mg acetaminophen) yields 20 mg x 1 (conversion factor) = 20 MME. That means that roughly either of these prescriptions taken for one month, once a year gets to the per capita MME of 640.
In addiction practice it is common to see people who are taking 120 to 240 mg/day of oxycodone per day. Doing the conversions yields a range of 180-360 MME. There is no good conversion from heroin to MME due to varied methodologies of use and very short half-life. With methadone the problem is long half-life and tolerance leading the conversion table to yield higher conversion factors at higher dose. With the calculations it was observed that the MME per capita peaked in 2010 at 782 MME and then decreased to 640 MME per capita in 2015. Both numbers are significantly higher than the MME per capita in the US in 1999 when it was 180 MME. Additional graphics of the other metrics from this article can be found in the tables below.
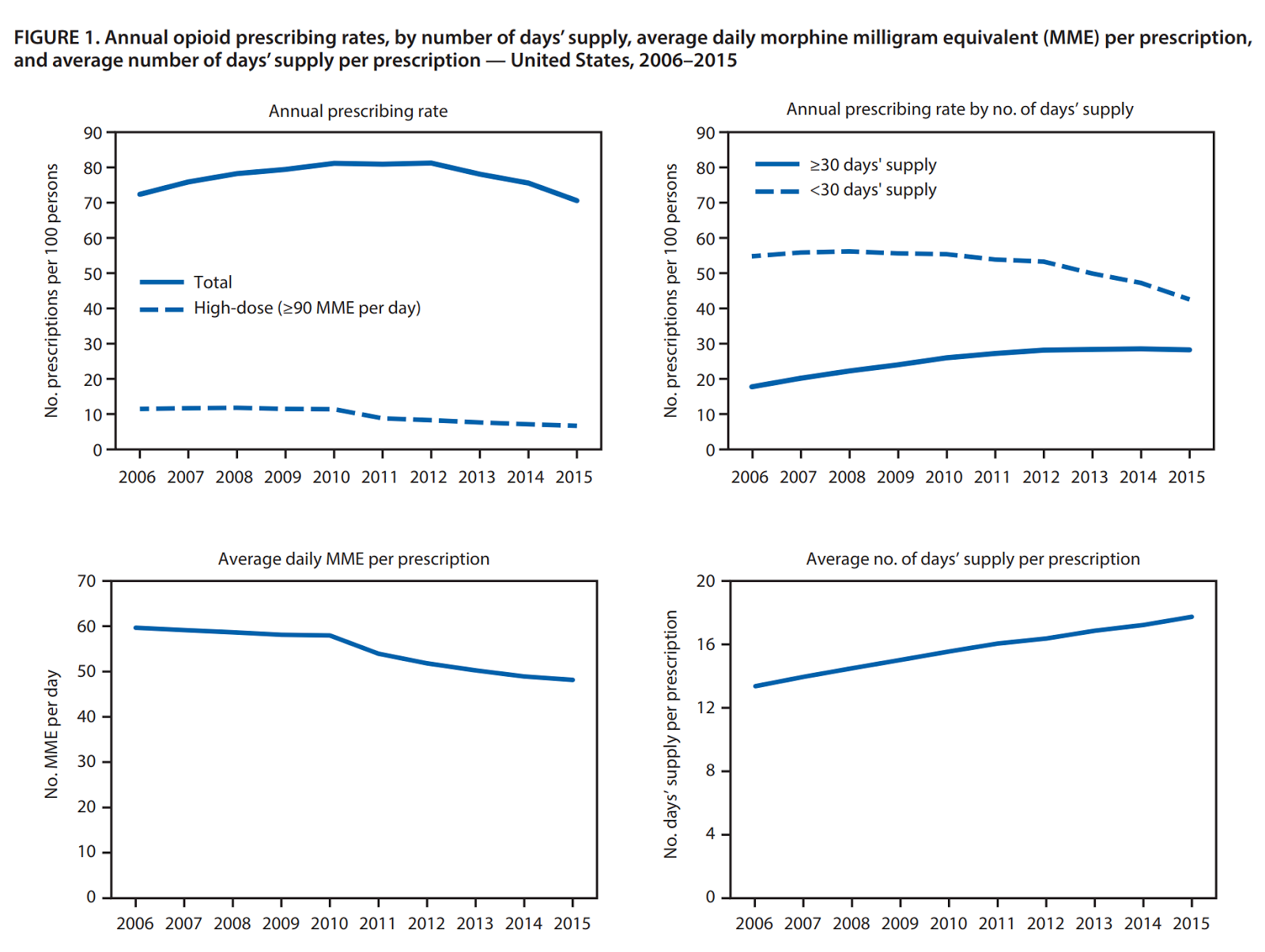
In the county by county assessment there were more decreased in overall prescribing rate (46.5%) and MME per prescription (49.6%) than stable or increased rates. The high dose prescribing rates dropped the most (86.5%). It is likely that guidelines describing the higher risk of high dose therapy affect these rates than the recognition of opioid use disorders in chronic pain patients. There was a significant increase in the average day per prescription in the county by county analysis (73.5%).
The authors also looked at a complex stepwise multivariable linear regression looking at numerous demographic variables and concluded that several variables accounted for higher amounts of opioids being prescribed including ( lower educational attainment, higher unemployment, more physicians and dentists per capita, higher prevalence of conditions associated with chronic pain (diabetes mellitus, arthritis, disability), higher suicide rates, and higher rates of uninsured and Medicaid enrollment. These variables accounted for 32% of the opioids prescribed at the country level.
The study has the expected limitations of a large retrospective database study. There are signs that that physician education and some regulatory action may be having an influence in opioid prescribing. Any reduction in the populations exposure to opioids would be expected to have some impact, but as of 2015 there were an estimated 2 million prescription opioid addicts (2). The recent transition from prescription opioids to heroin and some street products containing fentanyl and carfentanil has been responsible for an increase in opioid overdoses despite the change in prescribing patterns. Although the total opioid MME per capita has decreased it is still about 3 times higher than it was in 1999 - the year before the current epidemics inflection point. Proponents of liberal opioid prescribing might say (and have said) that the prescribing of opioids for chronic noncancer pain in the years leading up to 1999 was too stringent and deprived patients of needed pain relief. My experience with addiction suggests otherwise.
The risks of addiction with opioids is great. A current underemphasized area is primary prevention or not exposing young adults to opioids. The take home message from this paper is that secondary prevention may have an impact but at this point it is not clear cut. One thing is certain and that is the CDC does great work getting this data out and freely available to all interested physicians and patients in the world.
It will be a solid record of how the opioid epidemic evolved and hopefully at some point - resolved.
George Dawson, MD, DFAPA
References:
1: Guy GP Jr, Zhang K, Bohm MK, Losby J, Lewis B, Young R, Murphy LB, Dowell D.Vital Signs: Changes in Opioid Prescribing in the United States, 2006-2015. MMWR Morb Mortal Wkly Rep. 2017 Jul 7;66(26):697-704. doi: 10.15585/mmwr.mm6626a4. PubMed PMID: 28683056.
2: Substance Abuse and Mental Health Services Administration. Prescription drug use and misuse in the United States: results from the 2015 National Survey on Drug Use and Health. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2016. https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR2-2015/NSDUH-FFR2-2015.htm
Attribution: Both of the graphics in this post are from reference 1 above. Both are used per the user agreement for the MMWR that states this information is in the public domain.
Sunday, November 15, 2015
APA Misses On The Opioid Crisis - Several Times

The above infographic is courtesy of the CDC (see attribution for the direct link). To those of us involved in treating addictions talking with many people who are addicted to opioids, getting them to see the problem, and helping them prevent accidental overdoses and death is an everyday occurrence. The prescription opioid problem is widespread and has been a reality for the last 15 years even though it seems to have hit the news in about the last 5. That probably coincides with heroin use starting to escalate. The driving force for that has been economics. Heroin is generally available in most areas for about a quarter the cost of diverted prescription painkillers. In the past 5 years I have probably given about 50 lectures on the topic to physicians and graduate students and been actively involved in the clinical care of individuals with heroin addiction only or heroin addiction in addition to a number of other addictions.
When I got a post from the American Psychiatric Association (APA) on my Facebook feed last week it piqued my interest. Part of what I teach is how failed policy is the root cause of the opioid epidemic and what physicians can do on an individual basis to correct the problem. I was very interested to see what the APA had to say at a policy level. Reading through the document that is really a blog post from the Medical Director the answer is "not much". It appears that the APA has joined a Task Force of other professional organizations that includes that other great laggard the AMA. They will be working to identify "best practices" and implementing them as soon as possible. Using Prescription Drug Monitoring Programs (PDMPs) is encouraged. There will also be the focus on stigma. Dr Levin states: "The APA maintains that substance use disorder is a medical condition that can be successfully treated, and we are actively advocating on behalf of the patients who are too often stigmatized by their community and disenfranchised by insurance carriers who fail to comply with mental health parity laws."
While there is no doubt that most people are biased against people with mental illness and addictions as well as their psychiatrists - I don't think that stigma has any traction in terms of increasing access to care or more importantly access to quality care. I could argue that the APA support for the collaborative care initiative colludes with stigma-like biases. That takes the form of "you don't have to see a psychiatrist - take this checklist instead." I won't get into that today, only to say that I wonder how many people with heroin or opioid addiction are being seen in primary care clinics and being treated for anxiety, insomnia, or depression? From what I see the numbers are significant. But it is hard to fault primary care doctors because unless they are the prescribers of opioids, they may not realize that their patient has a problem with them. There is also the issue of institutional stigma versus public stigma. Public stigma or the type of stigma that everyday people have is more elastic and it usually depends on their experience with the problem. If you live in a family where a member has a severe mental illness or addiction - you know that these problems are real, life-threatening, and you are ready to let people know that. Institutional stigma is the type of stigma that governments and businesses can have, especially health care businesses. They might grudgingly admit that there is some kind of problem largely because there is such a large secondary impact on medical and surgical services. In some trauma centers over half of all admissions are primarily due to drug and alcohol problems. At the same time, institutional stigma is impervious to change. It is codified in some texts on healthcare management and as noted in the APA blog post - not even amenable to change when new federal parity laws are implemented. In terms of managing health care systems there is nothing like having a certain groups of disorders to shift resources away from in a pinch. Mental illnesses and substance use disorders are that group. The other considerations would include:
1. Irrational policy initiatives: There is no doubt that several policy initiatives to liberalize opioid prescribing were responsible for the start of this epidemic in or around the year 2000. Making pain the "fifth vital sign", encouraging the use of opioids for chronic non-cancer pain, treating minor conditions with opioids, and a widespread policy initiative that encourage more aggressive treatment of pain even though specific measures were not know are among these initiatives. I use the word irrational here to mean speculative initiatives that were not based on science.
2. A serious misunderstanding of the current problem: When all else fails blame physicians. That is a highly effective political strategy that worked to consolidate control of the health care system under business and government. To many of the politicians involved it flowed directly from their negative campaigning experiences. In this case, the opioid problem is being framed at some level as a problem of inappropriate prescribing by physicians. Some physicians are being subjected to criminal prosecution for deaths and complications that have resulted from opioid prescribing. There are no references to the policy changes that occurred in the late 1990's that led to this change in physician prescribing behavior - the loss of gate keep functions in particular.
3. A misunderstanding of the epidemiology of the problem: The upper decile of opioid prescribers (total number of prescriptions) account for 50-60% of all opioid prescriptions. These prescribers are almost all family physicians, internal medicine specialists, and mid-level prescribers. Available databases allow for rapid identification and intervention with these prescribers and that is where resources should be focused and not on all physicians across the board. A mechanism for feedback on an individual physician's or physician extender's ranking in terms of their prescription of controlled substances is needed as well as individual access to that information.
4. A serious misunderstanding for the overprescribing problem in general exists: As I have previously pointed out, opioids are one small group of medications that are overprescribed in the US. Practically everyone who wants this problem to go away sees it as a cognitive problem or knowledge deficit. If the physician involved just knew more they would not prescribe pain medications this way. In fact, it is a much more complicated interpersonal, social and intrapsychic problem for physicians. Until there is a widespread acknowledgement of this - all of the CME courses in the world on appropriate opioid prescribing will not change a thing.
5. There is a widespread cultural problem: Opioid hoarding in medicine cabinets across the country, neighbors sharing opioids and neighbors and family members discussing what is the best (translation best = most euphorigenic) is a major problem in the US. Many politicians have agreed that America's "insatiable appetite for illegal drugs" fuels the international drug trafficking problem. It also fuels the opioid epidemic. There are very few initiatives focusing on cultural change.
6. Misunderstanding the problems inherent in prescribing addictive drugs: Most physicians are not aware of the unconscious and conscious elements that are activated in susceptible individuals when they take addictive drugs. There are widespread misconceptions in this area that lead to the prescription of addictive drugs during active addiction, not assessing the risk of prescribing addictive drugs to a person in recovery, and failing to assess some of the indirect signs of addiction in patients who deny that they have a problem with addiction. There is also a belief among many physicians that if their goal is to help people that well intended prescribing will not lead to problems in the future.
These are 6 areas that the APA could be focused on. I don't think that you will see that analysis anywhere else. I expect that "best practices" will fall disproportionately on the average physician and be a waste of time on their time and energy. But it does fall back on the time honored political strategy of taking the heat off of the people who really failed and pretending it is a physician based problem.
George Dawson, MD, DFAPA
Attribution:
The infographic is from the CDC at this URL: http://www.cdc.gov/vitalsigns/heroin/infographic.html#use
The CDC has done great work in this area and their site should be closely monitored for new data relevant to the problem.
Subscribe to:
Posts (Atom)