The American Academy of Sleep Medicine (AASM) came out with a position statement about the use of medical cannabis for obstructive sleep apnea (OSA). In brief they think it is not a good idea. The entire statement can be read at the link. I think that it is important to keep in mind that they concerns about safety and efficacy are generally dependent on the fact that like most of the conditions on the Minnesota list, there is minimal to no scientific data to back up the suggested uses.
The AASM is not the first professional society to take a position on medical cannabis. One of the first purported applications of medical cannabis was for glaucoma. The American Academy of Ophthalmology has a position statement on Cannabinoids for Glaucoma that reviews the history of this application and concludes that although cannabinoids can lower intraocular pressure, the duration of this effect is too short and the side effect profile too problematic for cannabinoids to be used for this application. The statement points out that long acting cannabinoids for this application were recommended by the Institute of Medicine in 1999, but as of 2018 statement - there has been not suitable cannabinoid derivative.
That brings me back to the familiar refrain on this blog and that is the fallacy that cannabinoids or any street drug for that matter represents some form of miracle drug. Humans have been aware of cannabis for many applications for about 5,000 years. A reasonable question is why some miracle application or even one less than a miracle has not been found at this point in time. Why for example, were opioids developed as effective pain medications from the natural compounds over the same period of time? I have attended the lectures on physicians who advocate for medical cannabis. Some of them invoke Chinese medicine and quasi-scientific explanations like the entourage effect about why the whole plant needs to be smoked. I don't really see a need for physicians to certify people to access these largely unproven treatments, especially when medical colleagues are describing them as potentially unsafe and ineffective.
I have no problem with the state of Minnesota supplying medical cannabis to people with a condition that has no clear cut treatment. I have no concerns about the state supplying cannabis to people who are terminally ill. I do have a problem when cannabis is listed as a treatment when in fact there is little to no evidence that it is effective and vastly superior treatments exist. Glaucoma and obstructive sleep apnea are two of these conditions. From a purely psychiatric standpoint post traumatic stress disorder, and autism have existing treatments and autism has a newly approved treatment. In the case of Tourette's syndrome and other movement disorders - the data remains very preliminary.
As a prescribing physician, I have serious doubts about the thinking that goes into prescribing cannabis as an actual medication. I prescribe medications every day. These medications are all approved for use by the FDA. There are specific indications and off label uses. There are potentially serious side effects. The medications have to be prescribed to take the patient's chronic illnesses into account. For example, I would not prescribe a sedative to a patient who I thought might have obstructive sleep apnea. Prescribing cannabis, even in a special program that eliminates smokable cannabis continues to not make any sense to me.
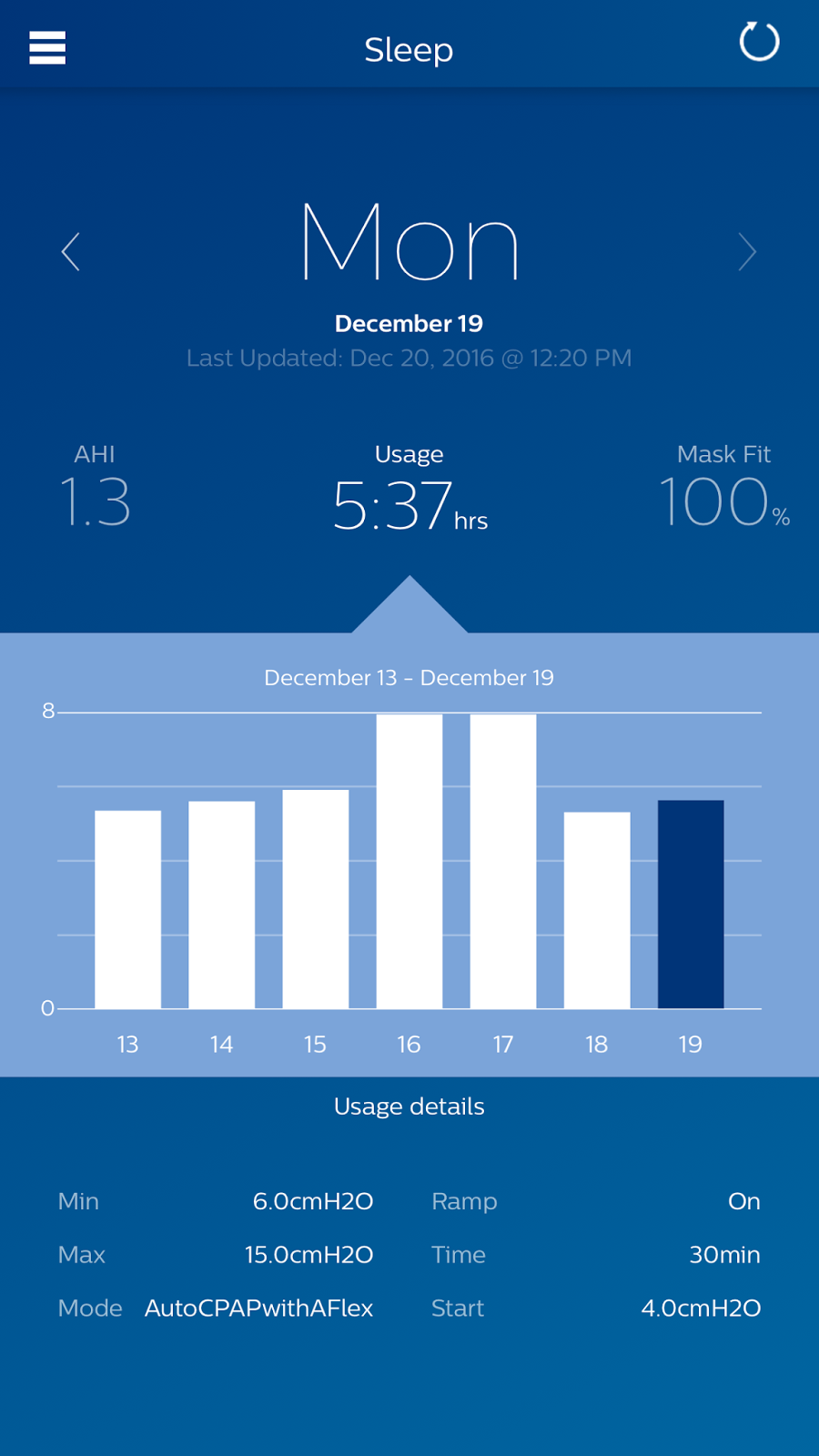
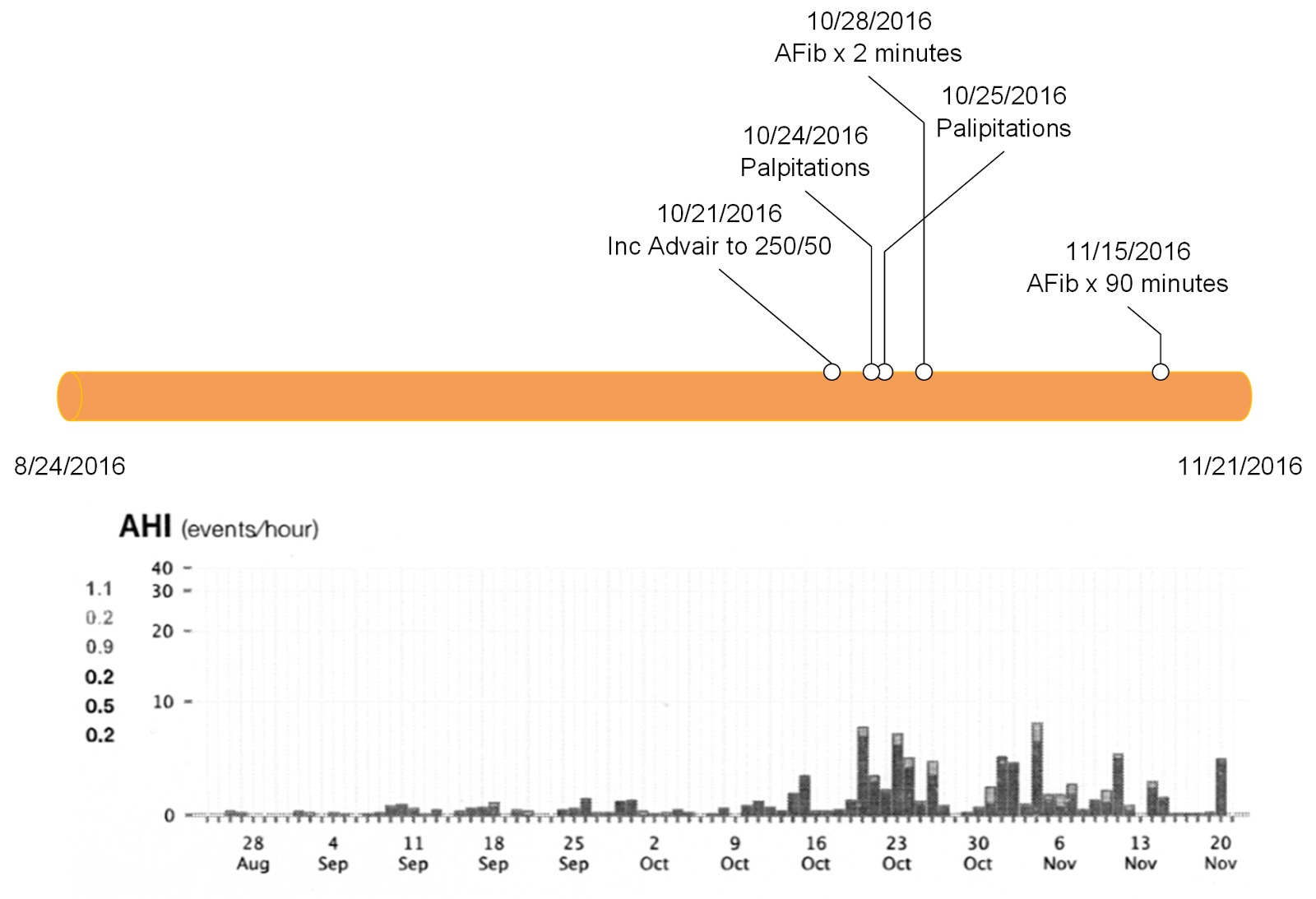
The list at the top of this page is directly from the Minnesota Medical Cannabis program as of today. It lists all of the current conditions that qualify a person to take it. I see the list as a political compromise to delay and potentially thwart the recreational marijuana movement. It should not be a surprise that medical cannabis has always been a mainstay of the strategy to legalize recreational marijuana. While that drama plays out - I hope that people in Minnesota don't forgo effective medical treatment for medical cannabis. Today that means CPAP for obstructive sleep apnea and glaucoma drugs and surgery for glaucoma.
There is no evidence that medical cannabis can come close to the medical effectiveness of those options. At the political level - this is also a great example of how politics negatively impacts quality medical care.
George Dawson, MD, DFAPA
References:
1: Ramar K, Rosen IM, Kirsch DB, Chervin RD, Carden KA, Aurora RN, Kristo DA, Malhotra RK, Martin JL, Olson EJ, Rosen CL, Rowley JA; American Academy of Sleep Medicine Board of Directors. Medical cannabis and the treatment of obstructive sleep apnea: an American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2018;14(4):679–681.
2: Petitions to Add Qualifying Medical Conditions to the Medical Cannabis Program. This document documents the review process for adding qualifying conditions to the list. Link
Graphic:
The table at the top of this post is directly from the Minnesota Medical Cannabis web site and is used here as a public document.