I bought a copy of Manic Depressive Illness when it first came out in 1990. One of the more interesting aspects of the book was the commentary on the use of lithium monotherapy for unipolar depression. That discussion is limited to about three pages and reviewed the work to date. In the opening paragraph there is this astonishing line: "Overall, the result of open studies suggest that lithium is as effective in preventing unipolar illness as it is in preventing bipolar illness." At the time there were 4 controlled studies (3-6) looking at the issue of maintenance therapy in mixed unipolar and bipolar groups. Three of the four studies showed no difference between groups. The fourth study was inconlusive due to a high dropout rate. Subsequent analyses by Schou and Baldessarini and Tohen concluded that the protective effects of lithium in preventing recurrent depressive episodes was good. In Schou's reanalysis he showed that the relapse rate in one year on lithium for unipolar depression was 22% (compared with a 20% relapse rate for bipolar disorder) and the rates for antidepressants at one year were 35% for unipolar depression and 65% for bipolar disorder (relative to placebo of 67-68% relapse rate).
Since that early open research there has been only randomized controlled clinical trial (RCT) of lithium versus placebo antidepressant augmentation (7). In that study 7/15 patients treated with placebo relapsed and one suicided. In the lithium treated group 0/14 relapsed. The authors recommended that patients who respond to lithium augmentation be maintained on it for at least 6 months. Additional clinical parameters of interest in the treated group was an average lithium dose of 980 mg, an average Li level of 0.65 mmol/L, and a response time of 17.5 days in acute treatment. This is interesting because many psychiatrists using lithium augmentation were taught to stop at 600 mg/day and accept the associated lower levels.
My point in the introductory paragraph here is that it has been known for some time that lithium may have a role in maintenance of unipolar depression in addition to bipolar depression - even though it is hardly ever used that way int he United States. In the US, patients typically endure a long series of antidepressant trials or augmentation strategies if the initial trails are ineffective. There is always the problems of whether the antidepressant has lost its effect or not and the associated difficulty of trying to determine what other factors may be operative. Lithium has been used for the past three decades as an augmenting agent - added to antidepressants. Typically a lower dose is used (600 mg/day) and that may offer a lower chance of toxicity and less need for monitoring blood levels.
Against this backdrop, a very interesting paper by Tiihonen, et al came out last year (2). For reasons that will follow, I consider this to be one of the most important papers for clinical psychiatrists from 2017. The authors provide a sound rationale for their study, specifically the advantages of a large scale epidemiological/observational study over an RCT or the Cochrane meta-analysis of RCTs. That meta-analysis (like most Cochrane meta-analyses) concluded that the number of subjects included was too small to come to a statistically significant conclusion.
The study was conducted in Finland. The authors point out that each citizen has a unique identifier that facilitates the design of large inclusive observational studies across health care databases. The sample in this case was a study cohort (N= 123,712) of patients who had been admitted to a hospital for unipolar depression between January 1, 1987 and December 31, 2012. They had a comparison incident cohort (N=30004) that looked at new patients beginning on December 31, 1996 with no mental health diagnosis, hospital admissions for depression, exposure to the medications of interest, or history of outpatient care in the year prior to the start. The purpose of the incident cohort was to look at the issue of survival bias. The primary outcome measure was risk of readmission in all patients admitted for unipolar depression at least once between 1987 and 2012. All cause admissions were a secondary outcome measure. Medication use was estimated using the PRE2DUP mathematical modelling of the patient medication purchasing. Each patient was used as their own control to eliminate selection bias. I did not have access to the appendices from this study, so I will forgo further discussion of the statistical methodology without that data.
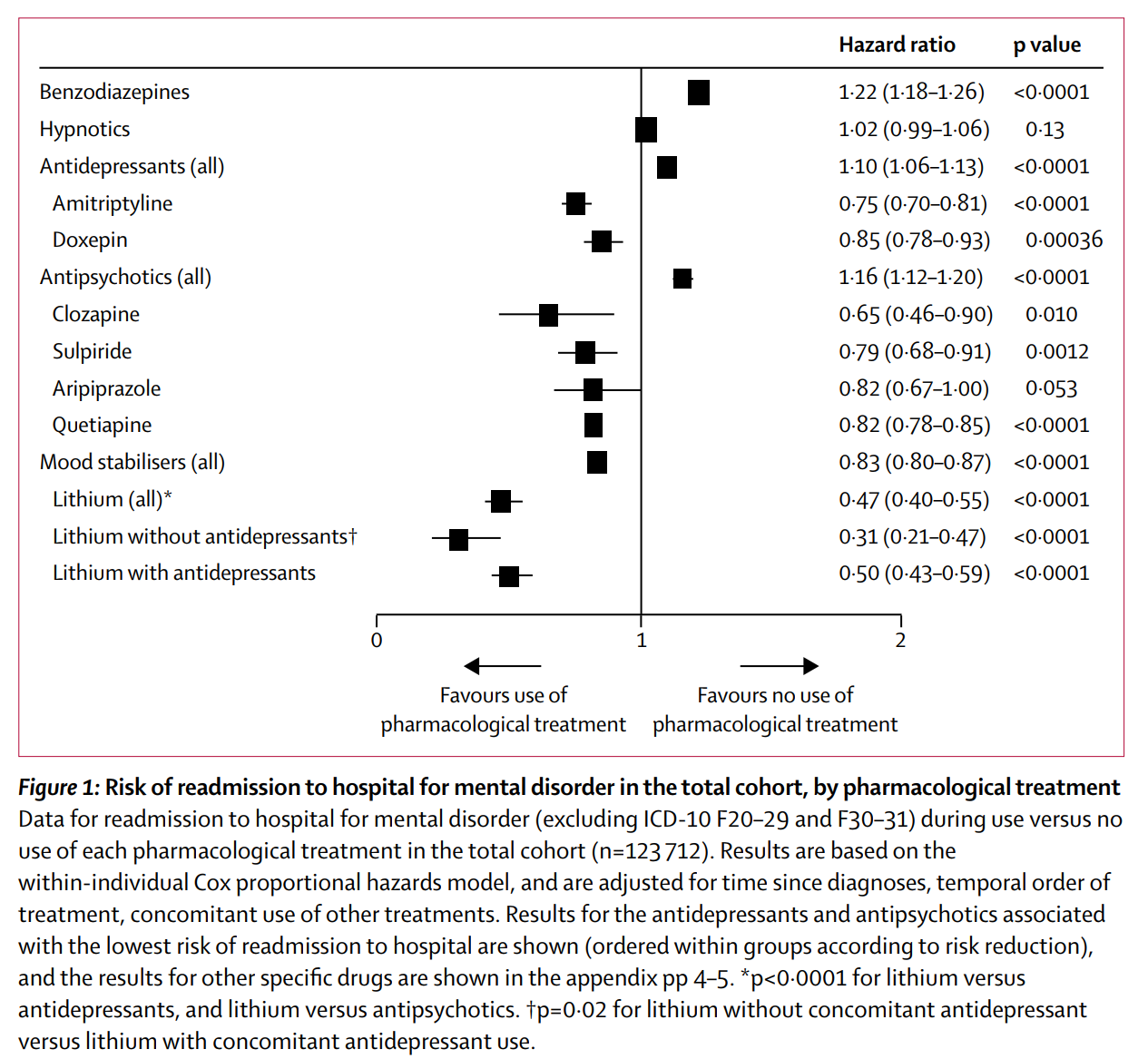
Mean hospitalizations for people who had used lithium was 4.3 (SD 6.9) for psychiatric admission and 7.8 (SD 9.1) for all cause admissions compared to 2.2(SD 3.1) and 5.8(SD 7.0) for those who had not indicating the lithium treated patient were more severely ill. Using lithium significantly decreased the relapse risk. Mean daily lithium dose was noted to be 765 mg. Forest plots are contained in the body of the article looking at the hazard rations of readmission for several pharmacological treatments in both the study cohort and the incident cohort. Forest plots looked at benzodiazepines, hypnotics, antipsychotics, and lithium +/- antidepressants.
Lithium monotherapy was superior to all other studied pharmacotherapies in preventing hospital readmissions. Older antidepressants (amitriptyline and doxepin) and antipsychotics (clozapine sulpride, aripiprazole, and quetiapine) showed some efficacy in preventing hosptializations. Benzodiazepines did not. In the incident cohort where (survival bias was eliminated) the lithium effect on decreased rehospitalizations was more robust suggesting the effect size was more valid than for the total cohort. They also did a secondary mortality assessment and showed that both lithium and antidepressants were associated with decreased overall mortality and no difference was observed for antipsychotics.
The authors recognize that there are significant adverse effects and limitations with the use of lithium. They point out there are also possible advantages outside the treatment of mood disorders but there is a significant burden associated with taking it. They recommend that is be considered for maintenance of a broader group of patients with unipolar depression. In our antidepressant-centric society, I agree with their conclusion. The effects in this study really cannot be ignored. Lithium augmentation of antidepressants has been around for over 30 years. It surfaced again the the STAR*D protocol. I see patients who have been exclusively been treated by other physicians or prescribers and in the past 8 years I have seen exactly 1 patient with unipolar depression who was being treated with lithium augmentation. It is far more common to see patient taking 2-4 antidepressants (typically SSRI + bupropion + trazodone or mirtazapine) or an antidepressant plus lamotrigine as the augmentation strategy. A similar study with a cohort of American patients would be very useful to look at questions about the efficacy of lithium versus the antidepressant polypharmacy or lamotrigine - but my concern would be that there would not be a large enough sample of patients taking lithium.
It may be up to clinicians who are used to lithium therapy and the application to unipolar depression to reintroduce the practice and collect data on what the outcomes are relative to standard antidepressant augmentation strategies. Overall this study from a group of pharmacoepidemiologists provides compelling data to take a second look at an old strategy instead of just adding more antidepressants. The data looks so good, lithium is so inexpensive, and in the USA we are in an absolute vacuum of lithium non-use for unipolar depression. Inpatient treatment for depression has become so atrocious that it has never been more important to help people stay out of the hospital. That is why I considered this to be an important paper.
George Dawson, MD, DFAPA
References:
1: Goodwin, FK, Jamison, KR. Manic-depressive illness. New York: Oxford University Press, 1990: pp.693-696.
2: Tiihonen J, Tanskanen A, Hoti F, Vattulainen P, Taipale H, Mehtälä J,Lähteenvuo M. Pharmacological treatments and risk of readmission to hospital for unipolar depression in Finland: a nationwide cohort study. Lancet Psychiatry. 2017 Jul;4(7):547-553. doi: 10.1016/S2215-0366(17)30134-7. Epub 2017 Jun 1. PubMed PMID: 28578901.
3: Prien RF, Klett CJ, Caffey EM Jr. Lithium carbonate and imipramine inprevention of affective episodes. A comparison in recurrent affective illness. Arch Gen Psychiatry. 1973 Sep;29(3):420-5. PubMed PMID: 4579507.
4: Prien RF, Caffey EM Jr, Klett CJ. Prophylactic efficacy of lithium carbonate in manic-depressive illness. Report of the Veterans Administration and National Institute of Mental Health collaborative study group. Arch Gen Psychiatry. 1973 Mar;28(3):337-41. PubMed PMID: 4569674.
7: Bauer M, Bschor T, Kunz D, Berghöfer A, Ströhle A, Müller-Oerlinghausen B.Double-blind, placebo-controlled trial of the use of lithium to augment antidepressant medication in continuation treatment of unipolar major depression. Am J Psychiatry. 2000 Sep;157(9):1429-35. PubMed PMID: 10964859.
Supplementary:
Figure 1 above is directly from reference 2 with permission from Elsevier. Licensing agreement #4270040486127.