"People in both camps seem to agree: We’ve had a big argument about health care over the past several years, yet we haven’t tackled the big issues. We haven’t tackled the end-of-life issues. We haven’t fixed the medical malpractice system. We are only beginning to correct the antiquated administrative systems."
And:
"... we haven’t addressed the structural perversities that are driving the health care system to bankruptcy. ... American health care is still distorted by the fee-for-service system that rewards quantity over quality and creates a gigantic incentive for inefficiency and waste."
The observations like essentially all observations about the ACA ignore the basic fact that this IS managed care and in fact - managed care on steroids. Managed care has proven time and time again to not contain costs and introduce administrative inefficiency in over two decades of experience. Whether or not the Supreme Court allows it to go forward or it is politically defeated in the future is peripheral to the fact that managed care has not worked as a device to contain health care inflation and it certainly does not provide either quality care or innovation. It can make money for stockholders and CEOs. In fact, in an up or down economy I can't think of a better recipe for making money than being able to deny health care benefits to a group of health care plan subscribers or deny or reduce reimbursement to physicians.
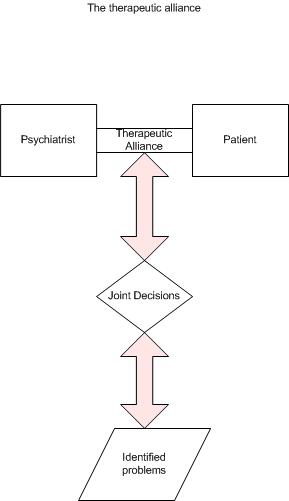
The structural perversity in the system is that in the overwhelming number of cases, personal health care decisions are no longer made between a patient and a physician. Contrary to managed care hype, their decisions are not necessarily based on any legitimate evidence. They are based on what is good for business and in this case we don't have a business that needs to build a better product. We have a business that has to ration access to a service.
Until that is recognized - health care reform is basically continuously rearranging ways to shift money from the people providing the care and the people paying for care to business entities that are "managing" the care.
The outcome is as predictable as where the managed care systems have gotten us to at this point.
George Dawson, MD, DFAPA
"... we haven’t addressed the structural perversities that are driving the health care system to bankruptcy. ... American health care is still distorted by the fee-for-service system that rewards quantity over quality and creates a gigantic incentive for inefficiency and waste."
The observations like essentially all observations about the ACA ignore the basic fact that this IS managed care and in fact - managed care on steroids. Managed care has proven time and time again to not contain costs and introduce administrative inefficiency in over two decades of experience. Whether or not the Supreme Court allows it to go forward or it is politically defeated in the future is peripheral to the fact that managed care has not worked as a device to contain health care inflation and it certainly does not provide either quality care or innovation. It can make money for stockholders and CEOs. In fact, in an up or down economy I can't think of a better recipe for making money than being able to deny health care benefits to a group of health care plan subscribers or deny or reduce reimbursement to physicians.
The structural perversity in the system is that in the overwhelming number of cases, personal health care decisions are no longer made between a patient and a physician. Contrary to managed care hype, their decisions are not necessarily based on any legitimate evidence. They are based on what is good for business and in this case we don't have a business that needs to build a better product. We have a business that has to ration access to a service.
Until that is recognized - health care reform is basically continuously rearranging ways to shift money from the people providing the care and the people paying for care to business entities that are "managing" the care.
The outcome is as predictable as where the managed care systems have gotten us to at this point.
George Dawson, MD, DFAPA