 |
| From: Reference 1 with permission. |
A friend of mine insists on telling me his dream. He knows I am interested:
"So I am in this old house. I have the feeling it is my Grandmother's house, but it is really a house I have never been in before. There is a gathering on the main floor and there are two people there. I know that one of them is supposed to be my grandmother but it doesn't look at all like her. There is a guy there who is apparently dating my grandmother. I know that he is supposed to be a handyman that my brother introduced to my Grandmother but I have never seen him either. They look like they are in their 70s. But in reality as you know - my grandmother has been dead for over 20 years."
"Suddenly I am no longer at the party. I am in the house and I am in an upstairs bedroom. For some reason, I think it is my grandmother's bedroom. I don't know why I'm there but all of a sudden this guy comes down the hallway. He is one of the commentators from TMZ that Hollywood gossip show (let's call him Bob). I look to the floor next to the wall to my right and there are two small bowls of M&Ms - a bowl of green M&Ms closer to him and a bowl of red M&Ms closer to me. They are in those Anchor Hocking glass bowls without the blue plastic lids. Anyway - I grab a small handful and start eating them. They are dark chocolate M&Ms. I look at Bob and say: "That's what they're there for" and he starts eating a few." He asks why I am there and I say: "I heard there was a mouse in here and I need to kill it."
"A mouse runs between me and Bob and I tell him to kill it. He misses it and it runs at me and I kick at it and knock it into the corner. Bob is still reluctant to kill it. The mouse runs at me again but this time it is as big as a rat. I kick it into the corner of the room again. This time it runs back out at me and it not longer looks like a rat - it is as big as an otter. I kick it again - but this time I am shaken awake by my wife. She asks me if I was having a bad dream. She said I was kicking my legs like I was running and punching my arms in the air for a few seconds. My heart was pounding like I was really in a fight with this thing. What was all of that? What does it mean?"
There are a few things about this dream that are striking. The first is the amount of detail recalled right down to what appear to be the product placements. Most people telling me about their dreams rarely recall this level of detail. Often they recall only the emotional tone of the dream and the vague idea that something happened. The second is the overall content of the dream. By the dreamer's report it is illogical - none of the events really happened or are likely to happen. With the exception of the TV celebrity, none of the people in the dream were really who they were supposed to be. Strangers were supposed to be his grandmother and his grandmother's boyfriend but in reality - there was no such relationship. There is the movement. The dreamer is thrashing about the bed until his wife wakes him up. A final consideration that I like to think about is the processing power necessary to create this experience either de novo or from existing elements.
Dream interpretation is still alive and well in psychiatry - at least the way I practice it. It is not quite the detailed analysis of all of the elements that Freud thought were important but a combination of a look at the predominate affects and what might be called a synthesis of what is supposed to happen in dreams. It is also not quite where we need it to be from a neuroscientific perspective. For example, for the most part we are still operating on a model that suggests more dream activity occurs in REM (rapid eye movement) sleep and that NREM (non-rapid eye movement) sleep contains very little. We know from dream studies that is not completely correct because both REM and NREM sleep have EEG correlates and we can wake research subjects up during dreams and determine if they are dreaming or not. Based on those studies there is a rough correlation - but there are still dreams occurring during NREM sleep and REM sleepers without dreams. Various theories have been advanced about why that occurs, but there is no comprehensive theory. The other issue is that dream content needs a better explanation. The simplified explanation is that illogical impossible dreams like the one described here are REM dreams and that NREM dreams are more like plausible events. Finally - movement during REM dreams is not possible suggesting that the dreamer in the above example was not in REM sleep or he has a neurological problem to account for the dissociation between his motor activity and the fact that he should be paralyzed in REM sleep. These thoughts about REM and NREM sleep are so pervasive in our society that I routinely interview patients who tell me why they think they are (or are not) getting enough "REM sleep".
I was lucky to have found a recent paper (1) on the subject that if correct may prove to be a landmark study about the neural basis of dreaming and possibly consciousness. One of the advantages of this paper is that is it written from the perspective of consciousness researchers with an interest in the neural correlates of consciousness. In this study the authors ran three experiments looking at the question of dream reports and high density (256 channel) EEG. They used a serial wakening model in which subjects were awakened and asked to report if they were dreaming and could recall some of it (DE = dreaming experience) or if they experienced something but could not recall (DEWR=dreaming without recall of content). A third option was no experience of dreaming (NE = no experience). They were asked to characterize any content further according to protocol. There were two groups of research subjects. The first was a group of 32 subjects who underwent few awakenings - 233 total. The second was a smaller group of 7 subjects who had many (815) awakenings. In a third experiment 7 subjects were studied with 84 awakenings to see if the results of the first two experiments could be predicted.
The initial section of the paper reports on the results of DE versus NE experience in the low frequency (1-4 Hz) power spectrum. The authors were able to identify what they describe as a posterior cortical hot zone (bilateral parieto-occipital area including the occipital lobe extending to the precuneus and posterior cingulate gyrus superiorly p. 873). DE occurred when there was decreased low frequency power in this region. That condition occurred in both REM and non-REM states. This finding across distinct sleep stages appears to be highly significant.
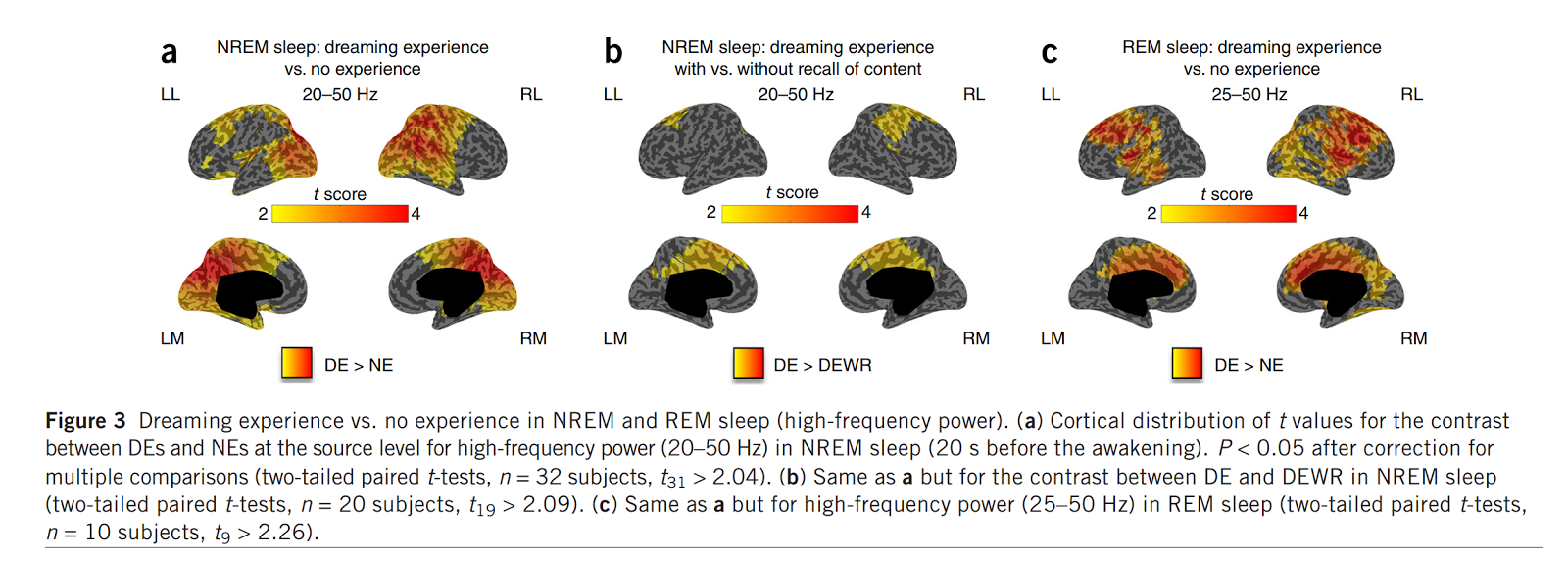
The next section of the paper reports on DE versus NE in the high frequency power spectrum (20-50 Hz) that corresponds with high rates of neuronal firing. Some of the results are summarized in Figure 3 at the top of this post. In the DE experience condition increased high frequency power was noted in the same parieto-occipital regions that were associated with decreased low frequency power but it was more extensive. DE with recall of content was associated with more widespread extension of the high frequency map than DEWR (no recall of content). Additional observations were made of the high frequency maps with regard to specific recalled dream content. The results here are extremely interesting in terms of the specifics of content. The authors comment on the "perception versus thought" content of dreams. Some recalled content is an isolated thought or emotion and other content is very vivid imagery including full conversations like the example at the top of this post. In their experiments, the authors note that there appears to be an anterior -> posterior gradient for high frequency activity with thought content mapping out over frontal cortex and perceptual content mapping out over posterior cortical regions. They looked at dream content involving facial recognition and noted an increase in high frequency activity over the right fusiform gyrus - a structure noted to be involved in facial recognition during wakefulness. Dream content that involved spatial imagery was correlated with increased high-frequency activity in the right posterior parietal cortex and area with that expected function during wakefulness. Additional correlations were noted with movement and speech.
In the final phase of the experiments, the authors sought to find out if the markers identified in the initial sections of the paper could be used to predict where or not a person was dreaming just based on their EEG data. They were able to accurately predict dreams 80.7 to 91.6% of the time (87% accurate across all states).
I consider this to be a potentially critical paper to any psychiatrist interested in sleep or dreaming. If replicated it illustrates that there is a posterior cortical hot zone that correlates with dreaming across REM and NREM sleep stages. That in itself explains the lack of tight correlation of dreams with REM and NREM sleep. From a theoretical standpoint they point out the the low delta activity (1-4 Hz) that correlates with dreaming also corresponds to alternations in neuronal depolarization and hyperpolarization that causes a breakdown in cortical communication. High delta activity corresponds to states of diminished consciousness including some forms of delirium and loss of consciousness. They suggest that posterior cortical activation should be studied in patients with disorders of consciousness to see if there may be consciousness without responsiveness based on activity in this area. They also discuss the broader implications of dreaming as a model for the study of consciousness.
That is a good point to end this post. I will continue to monitor the work of these authors and have been following some of them for some time. Dr. Tonini for example is probably one of the top experts (and theorists) on consciousness and the only psychiatrist who I am aware of who is doing this work.
George Dawson, MD, DFAPA
References:
1: Siclari F, Baird B, Perogamvros L, Bernardi G, LaRocque JJ, Riedner B, Boly M,Postle BR, Tononi G. The neural correlates of dreaming. Nat Neurosci. 2017 Jun;20(6):872-878. doi: 10.1038/nn.4545. Epub 2017 Apr 10. PubMed PMID: 28394322; PubMed Central PMCID: PMC5462120
Attribution:
Figure 3 at the top used with permission from Nature Publishing Group - License Number 4154981341951. The figure is from reference 1.
Supplementary:
As I have previously posted - I have experience with standard array quantitative EEG (QEEG) and its limitations. I am a little skeptical of being able to determine the EEG spectrum in the fusiform gyrus by standard surface electrodes in what I imagine is a cap array. But time will tell.